
If you don’t have a PhysioOutcomes account, sign up here:
If you have an account and forgot your password, click here:

PHYSIOOUTCOMES IS A TECHNOLOGY PLATFORM THAT ENGAGES YOU IN PREVENTING MUSCULOSKELETAL INJURIES, AND IF YOU SUSTAIN AN INJURY, FACILITATES YOUR ACTIVE INVOLVEMENT IN THE RECOVERY PROCESS.
THIS STRATEGY INCLUDES ACCESS TO OUR eREHAB PLATFORM TO HELP ENGAGE YOU DAILY FROM INJURY TO YOUR RECOVERY. WE HAVE PHYSIOOUTCOMES PATHWAYS FOR ALMOST EVERY ORTHOPEDIC PROBLEM.

BY OFFERING RESOURCES FOR BOTH PREVENTING AND RECOVERING FROM INJURIES, PHYSIOOUTCOMES ALLOWS YOU TO PARTICIPATE IN YOUR CARE WHICH HELPS YOU RETURN TO WORK, SPORTS AND NORMAL LIFE SOONER.
Prospective multiple case study analysis
Presented at The 2014 American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting in New Orleans, Louisiana
Internet Enhanced, Patient-Centered Orthopedic Care:
A Prospective, Randomized, Controlled Pilot Trial
Jonathan Paul, MD ,Kasey Rolfes, DHA, MS, ATC-L,Bryan Herron, MD
Charlotte Sports Medicine Institute, Charlotte, NC and Advanced Orthopaedic Specialists, Prince Frederick, MD
Presented at The 2015 American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting in Nevada, Las Vegas
Abstract
Objective: We have developed a patient-centered web portal that utilizes streaming, clinician prescribed video instruction to motivate and inform patients in self-care of their orthopedic condition, focusing on the importance of a home exercise program. The objective of this study is to compare this web portal (eRehab) to formal outpatient physical therapy (PT) in terms of patient costs and outcomes. Our hypothesis is that in certain patient populations, eRehab will yield similar clinical outcomes to PT and provide significant financial savings to the healthcare system.
Study Design: This is a multicenter, prospective, randomized controlled pilot trial.
Setting: Private practice orthopedic surgery clinics.
Patients: Twenty patients with an initial pain score less than 6 who were diagnosed by a board certified orthopedic sports medicine surgeon who were candidates for a knee or shoulder orthopedic outpatient physical therapy referral. Seventeen patients completed the study.
Interventions: Patients were randomized to a six-week treatment course of either standard PT or eRehab.
Main Outcome Measures:Patients were evaluated for outcome scores (Dash or Reverse KOOS), pain NRS-11 scores, patient subjective outcomes, and cost of treatment for the current episode of care.
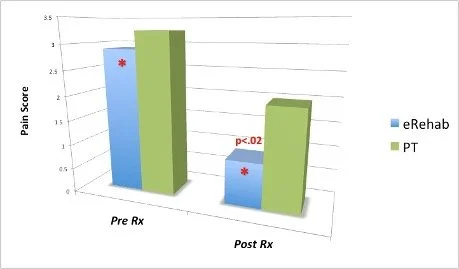
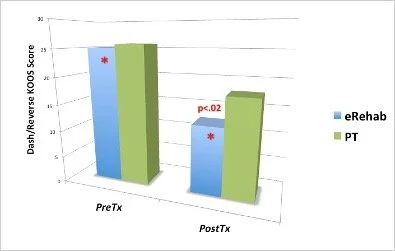
Results: At the six-week follow-up evaluation, only the eRehab group achieved a statistically significant improvement in both pain scores (2.9 v .9, p = .02)
and outcome scores (25.1 v 12.6, p <. 02).
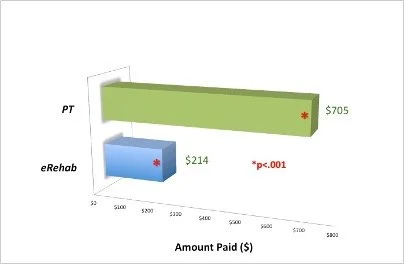
Patients who were candidates for an outpatient physical therapy referral who instead were treated with an eRehab treatment plan had a significant reduction in total cost of care per episode ($214 v $705, p < .001)
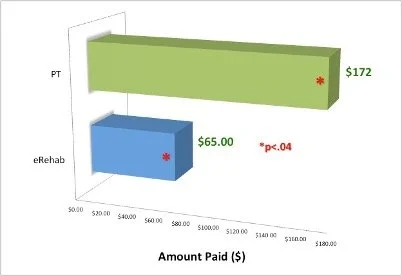
and patient cost per episode ($65 v $172, p < .04).
Conclusions: The outcomes of this pilot study suggest that Internet-based home exercise programs may be a viable option to standard physical therapy for knee and shoulder patients with a pain score less than 6.
A Prospective multiple case study analysis
Jonathan Paul, MD ,Kasey Rolfes, DHA, MS, ATC-L,Bryan Herron, MD
Charlotte Sports Medicine Institute, Charlotte, NC and Advanced Orthopaedic Specialists, Prince Frederick, MD
Presented at The 2014 American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting in New Orleans, Louisiana
Initially, to evaluate patient interaction with WebHSR rather than to make comparisons with clinical physical therapy, we reviewed the first 10 cases randomized to the eRehab intervention. Cases were examined individually through program views, exercise logs, survey and questionnaire results, and outcomes based on patient reports and physician evaluation notes. The results of the individual analyses were collectively summarized and reviewed for trends. Results of qualitative data interpretation were verified by a separate review and analysis by an academic medical professional not affiliated with the study
Each individual patients utilization of the platform is listed below followed by Table 1 which lists demographics, web portal utilization and outcome scores for the first 10 patients randomized to the eRehab group.
Individual Patient Data:
Patient A
Patient B
Patient C
Patient D
Patient E
Patient F
Patient G
Patient H
Patient I
Patient J
dATA FROM Physiooutcomes -rETROSPECTIVE sTUDY
To get an initial assessment of patient utilization of PhysioOutcomes, we performed a retrospective review of 289 consecutive eRehab prescriptions from a single orthopedic clinic. Most patients viewed the patient education videos in the office and all were prescribed an eRehab prescription allowing them the opportunity to log on at home for free to watch the videos as many times as they needed to gain an understanding of their condition and how to do their exercises properly. All major orthopedic conditions and body parts were included in this retrospective review. ANOVA and independent Student’s t-test were applied to the data to compare patient demographics with the number of eRehab logons and website utilization.
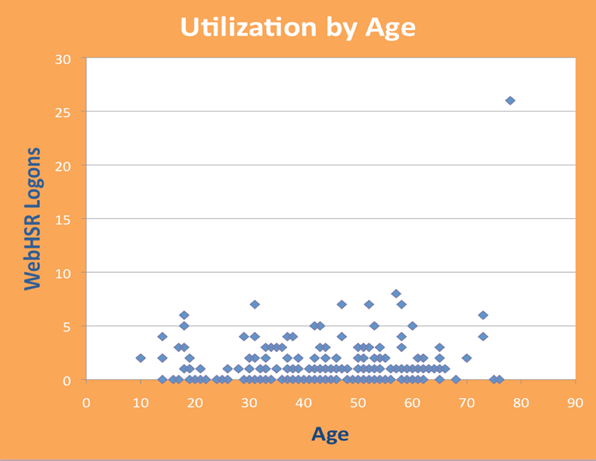
One hundred and seventy-one patients viewed their prescription at home at least once for an overall patient home view rate of 60%. There were 1.31 home views per patient (range 0 - 26). For the 171 patients who viewed their prescription at home at least once, the average number of home views was 2.22. There was no correlation between patient age (Figure 1), sex or type of health insurance with utilization of the web portal.
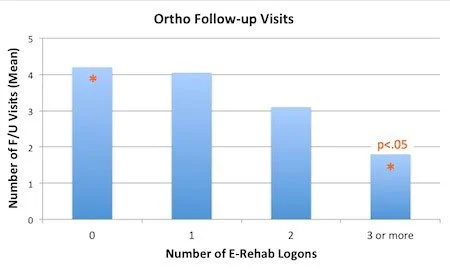
Figure 2
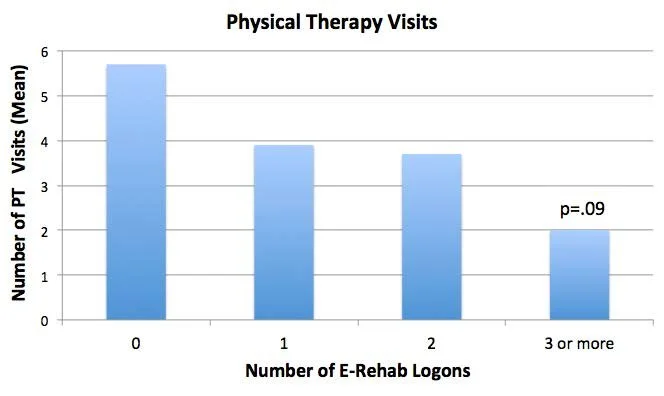
A similar trend (Figure 3) was seen for the number of outpatient PT visits for the current diagnosis.
A statistically significant reduction in mean number of orthopedic follow-up visits for the current patient’s current diagnosis (Figure 2) was seen between patients who viewed the videos three or more times at home (1.8 follow-up visits) compared to patients that never viewed the videos at home (4.2 follow-up visits) (p<. 05, Student t-test).
Figure 3
pilot study at Group Health Cooperative
Seattle, WA
We performed a pilot study at Group Health Cooperative in Seattle, WA.
Seven primary care, sports medicine fellowship trained MDs and 1 sports medicine fellowship trained orthopedic surgeon prescribed PhysioOutcomes eRehab to 178 non-operative, patients.
An 80% patient view rate of the exercise and patient education videos was achieved with no adverse encounters.